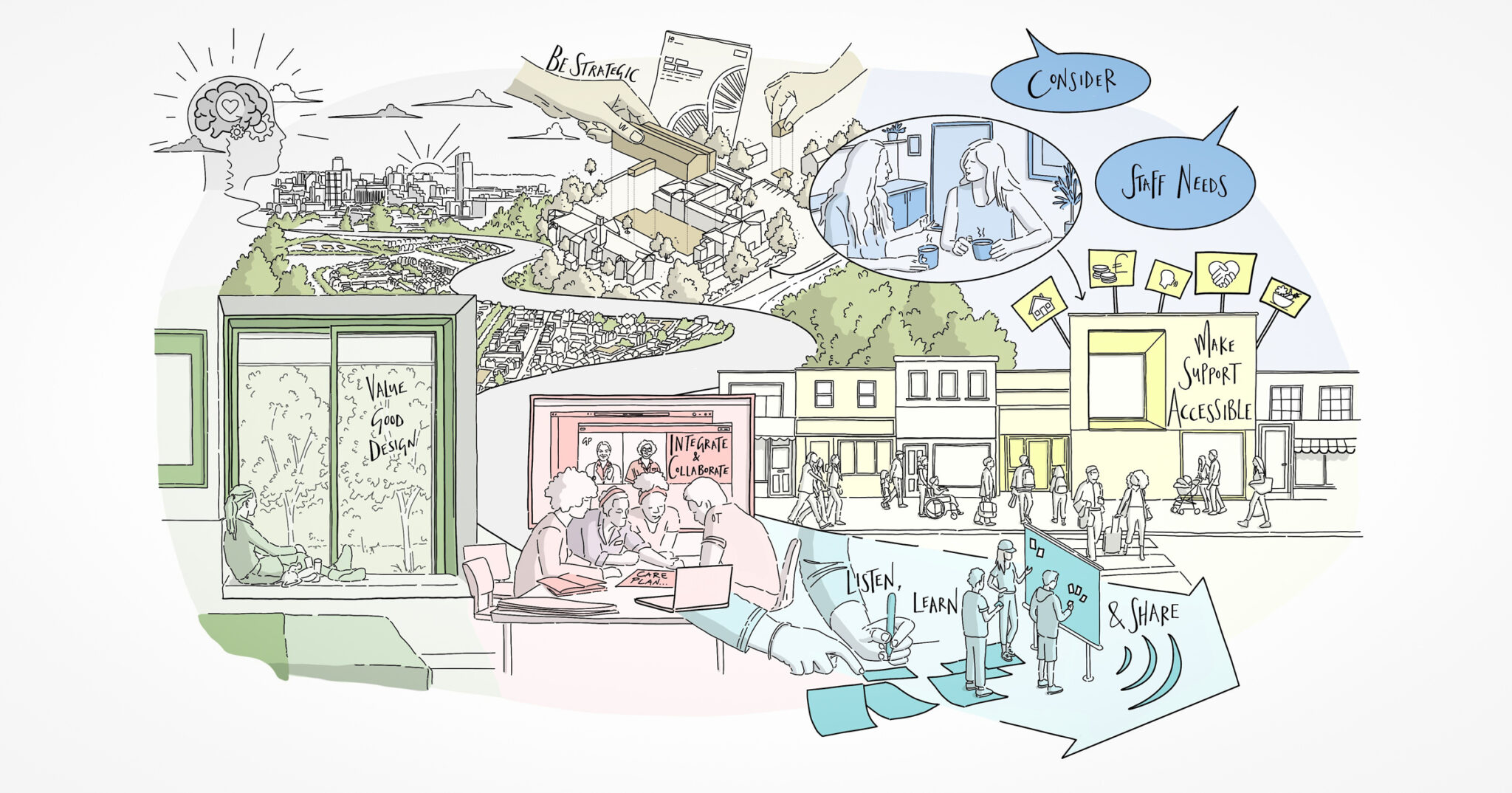
Learn from successful models of integration to provide more holistic and preventative care, and design buildings that support collaboration.
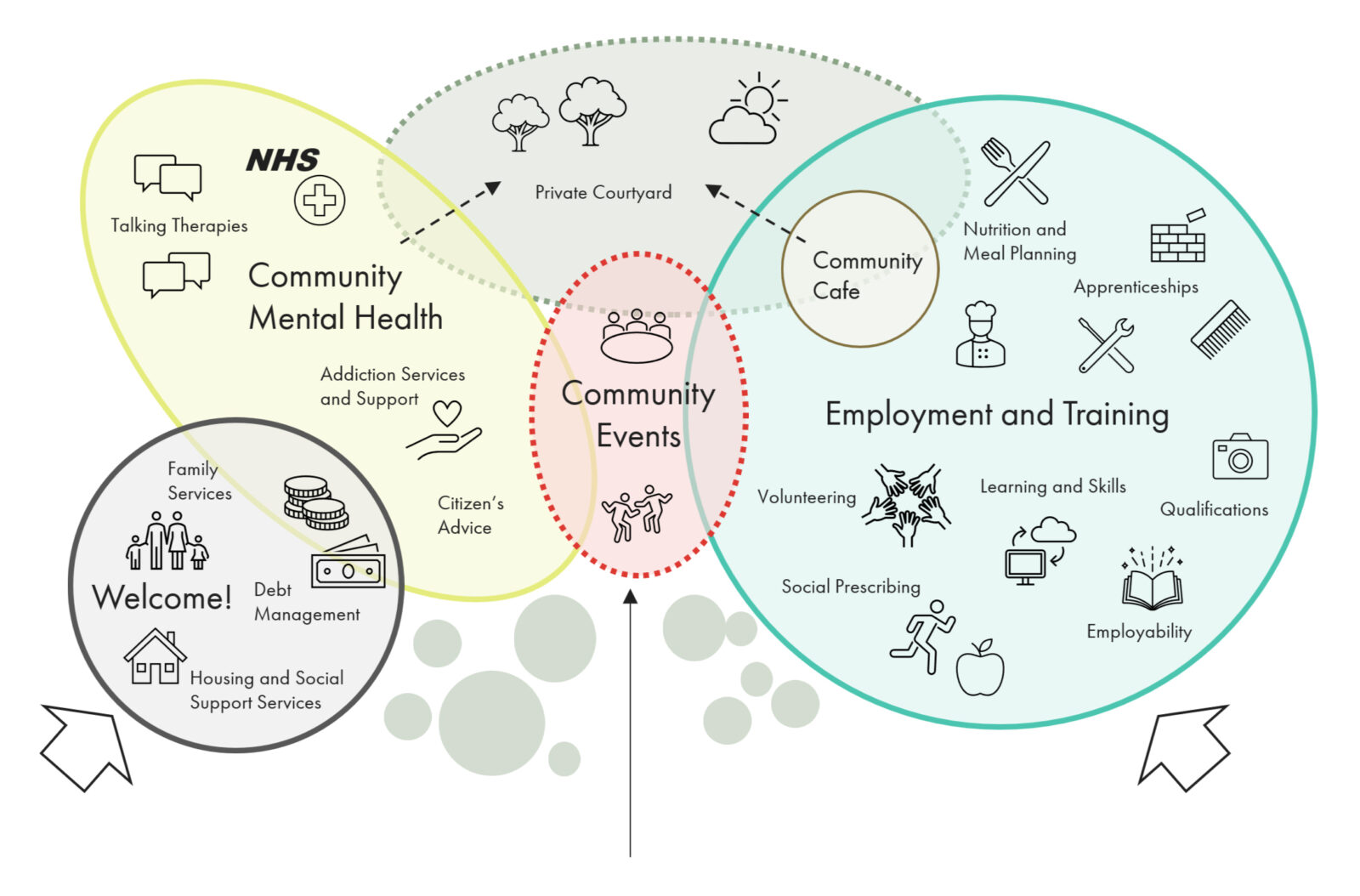
Our group was in agreement that greater collaboration between health organisations is needed to provide more integrated services, where patients are treated as a whole person and not several compartmentalised challenges. This represents a more relational way of delivering mental health care, as opposed to transactional responses to individual issues. One of our participants shared a comparison to being treated by cancer services, where treatment was fully holistic, from day one on the pathway, an experience that is worlds away from their experience of mental health services.
Innovative international models of care were discussed as potential sources of inspiration for a more relational approach, including the Trieste model in Italy. The Trieste model originated in the 1970s under psychiatrist Franco Basaglia, and it revolutionized mental health care by transitioning from institutionalisation to community-based services. It emphasises holistic, person-centered care, integrating individuals with mental health conditions into society (see accompanying case study).
We know it works, but it does feel that implementing it in the UK has a way to go yet. For it to work here, we need to plan – the strategic point again – for integration and holistic care. It isn’t enough to combine services in a building and expect collaborative working to flourish, we need to plan how services should integrate and what that means for the patient journey and building design.
The NHS 10 Year Health Plan and a shift to a ‘Neighbourhood Health Service’ provides a positive indication of future plans. As does the first batch of 24/7 neighbourhood mental health centres which are being rolled out across the country. But the detail around implementation is important, as is sufficient funding to ensure success. However, examples such as the Trieste model show that new models of service delivery can achieve long term cost savings if prioritised.